Complex Coronary Angioplasty, Rotablation, and IVL
When a Standard Stent Is Not Enough: Advanced Techniques for
Difficult Blockages
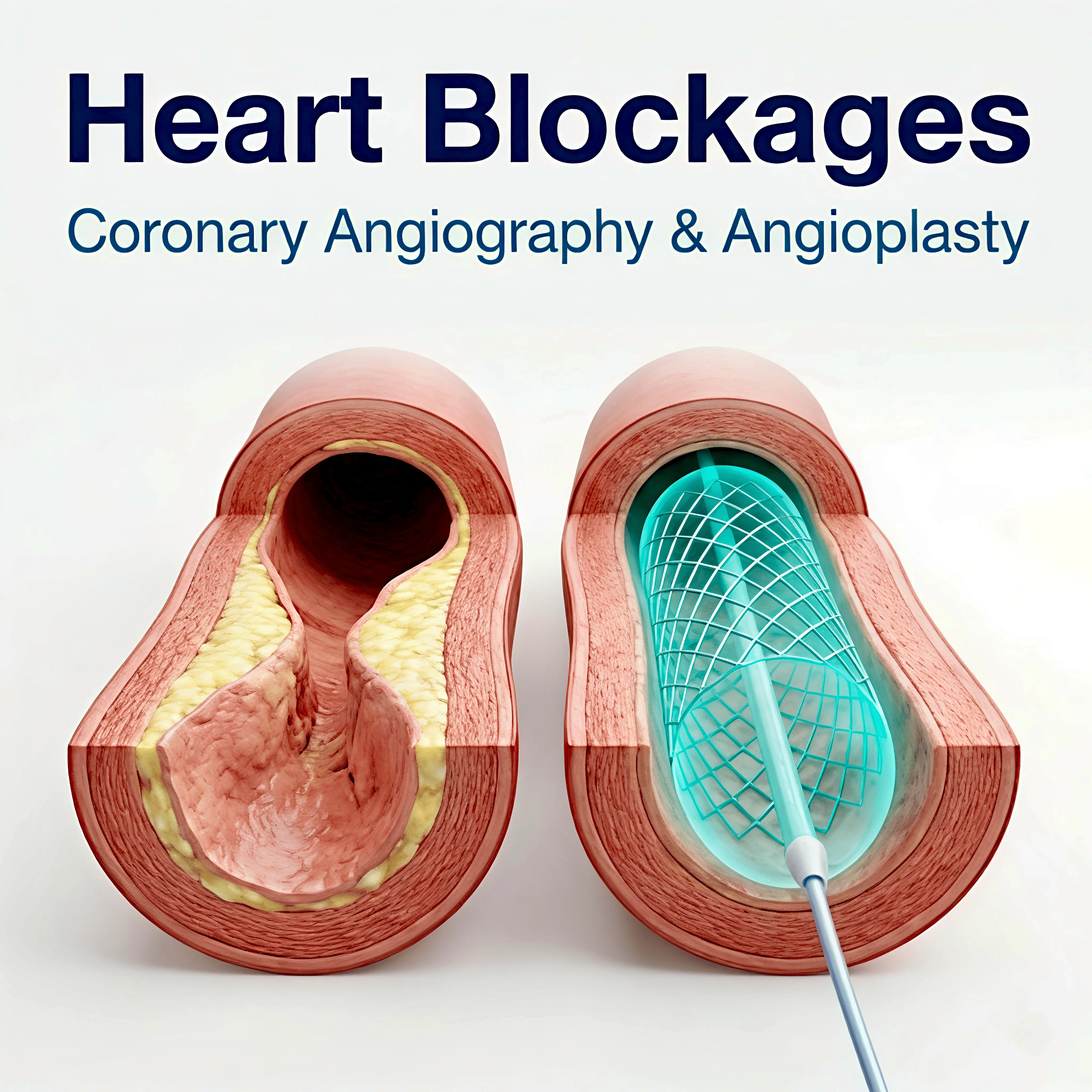
Not every heart blockage can be treated with a standard balloon and stent. Some blockages, particularly those that have been present for years, become heavily calcified. The artery wall hardens almost like bone, making it impossible to open with a conventional balloon. Two advanced techniques have changed what is possible for these patients: rotational atherectomy (rotablation) and intravascular lithotripsy (IVL).
What
Makes a Blockage 'Complex'?
A blockage is considered complex
when one or more of the following apply: it is heavily calcified (hardened with
calcium deposits); it is a chronic total occlusion meaning the artery has
been completely blocked for months or years; it sits at a bifurcation point
where the artery branches; or it involves a long segment of the artery rather than
a short focal point.
These blockages require more
advanced planning, more specialised equipment, and greater procedural
experience than routine angioplasty. They are the cases that define the
difference between a general interventional cardiology programme and a highly
experienced one.
What Is Rotablation?
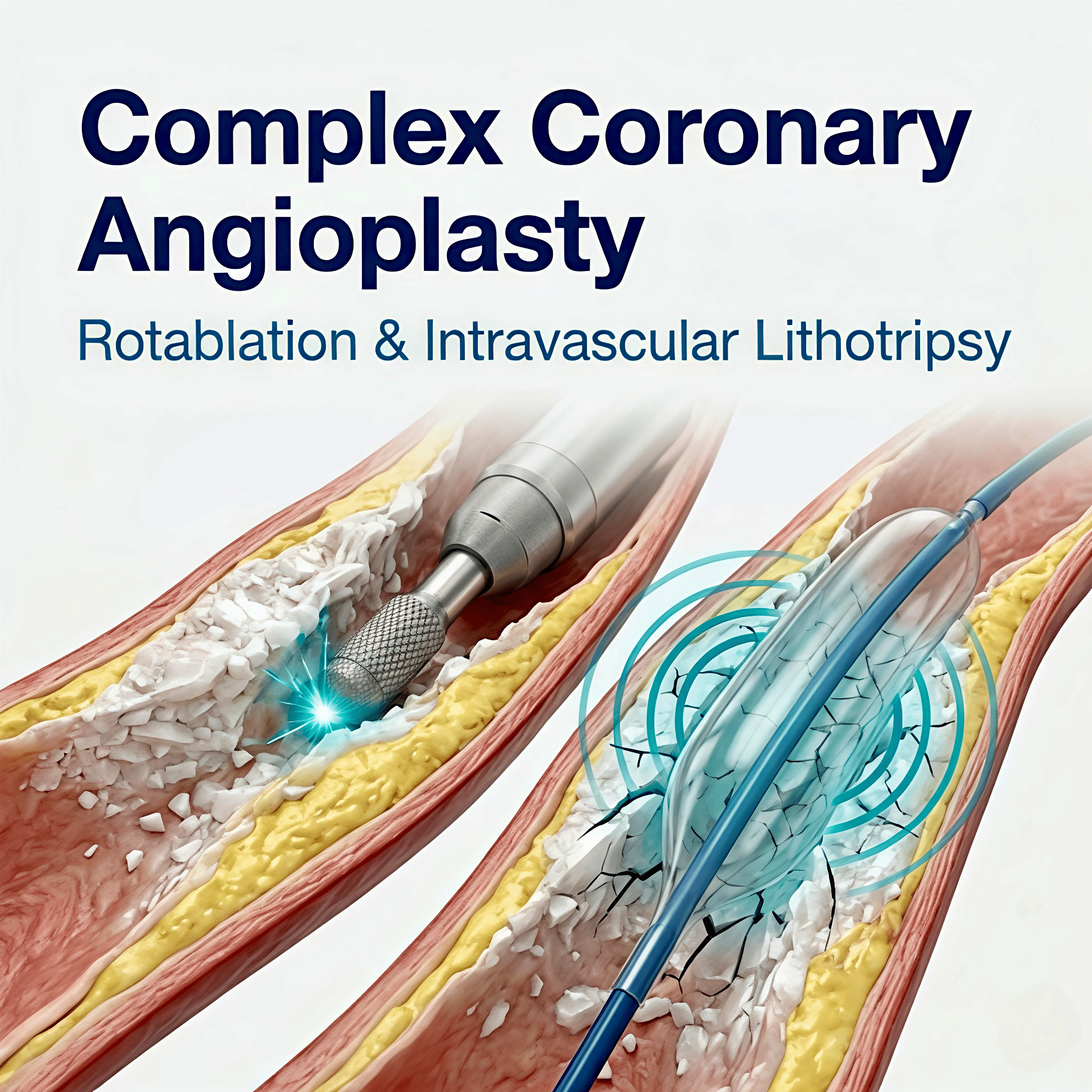
Rotational atherectomy rotablation uses a tiny diamond-tipped burr that spins at very high speed and
is advanced along a guidewire to the site of the calcified blockage. The burr
grinds away the hardened calcium, breaking it into microscopic particles that
are cleared safely by the body. Once the calcium is debulked, the artery can be
dilated with a balloon and stented in the usual way.
Rotablation does not remove the
entire blockage; it modifies it enough to allow safe stent delivery. The
result is a properly expanded stent in an artery that could not previously
accommodate one.
What Is Intravascular Lithotripsy (IVL)?
Intravascular lithotripsy IVL uses a different approach. A specialised balloon is delivered to the site of
the calcified blockage. Inside the balloon, sonic pressure waves are generated
that crack the calcium deposits within the artery wall, making it pliable
enough to accept a stent. Unlike rotablation, IVL does not remove tissue; it
fractures the calcium in place.
IVL is particularly well-suited to
calcium that sits deep within the artery wall rather than projecting into the
vessel lumen. In some cases, it is used alongside rotablation or independently,
depending on the nature of the calcium.
Who Needs These Procedures?
These are not everyday procedures.
They require specialist equipment and significant experience. Apollo CVHF's interventional cardiology team performs complex coronary interventions, including rotablation and IVL, regularly.
•
Patients with heavily
calcified blockages where a standard balloon cannot be fully inflated
•
Patients whose previous
stent cannot be re-expanded due to calcium
•
Patients with chronic total
occlusions requiring complex wire crossing techniques
•
Patients who have been told
their blockage is 'too difficult' or 'not suitable' for angioplasty elsewhere
What Should I Expect?
The procedure is performed in the catheterisation laboratory, through the wrist in most cases, under local anaesthetic and sedation. It typically takes longer than routine angioplasty, often between 1.5 and 3 hours, depending on complexity. Most patients stay overnight and go home the following day.
|
If
you have been told elsewhere that your blockage cannot be stented or that
the procedure is too high-risk, bring your angiography CD to Apollo CVHF for
a review. A second assessment is always worthwhile. |