Heart Blockages, Coronary Angiography, and Angioplasty
Understand Your Blockage. Know Your Options. Decide With
Confidence.
A heart blockage - a narrowing
inside one of the coronary arteries is one of the most common cardiac
diagnoses. It is also one of the most commonly misunderstood. Not every
blockage on an angiogram needs a stent. Not every patient told they need
angioplasty actually does. Understanding the difference starts with getting the
right assessment.
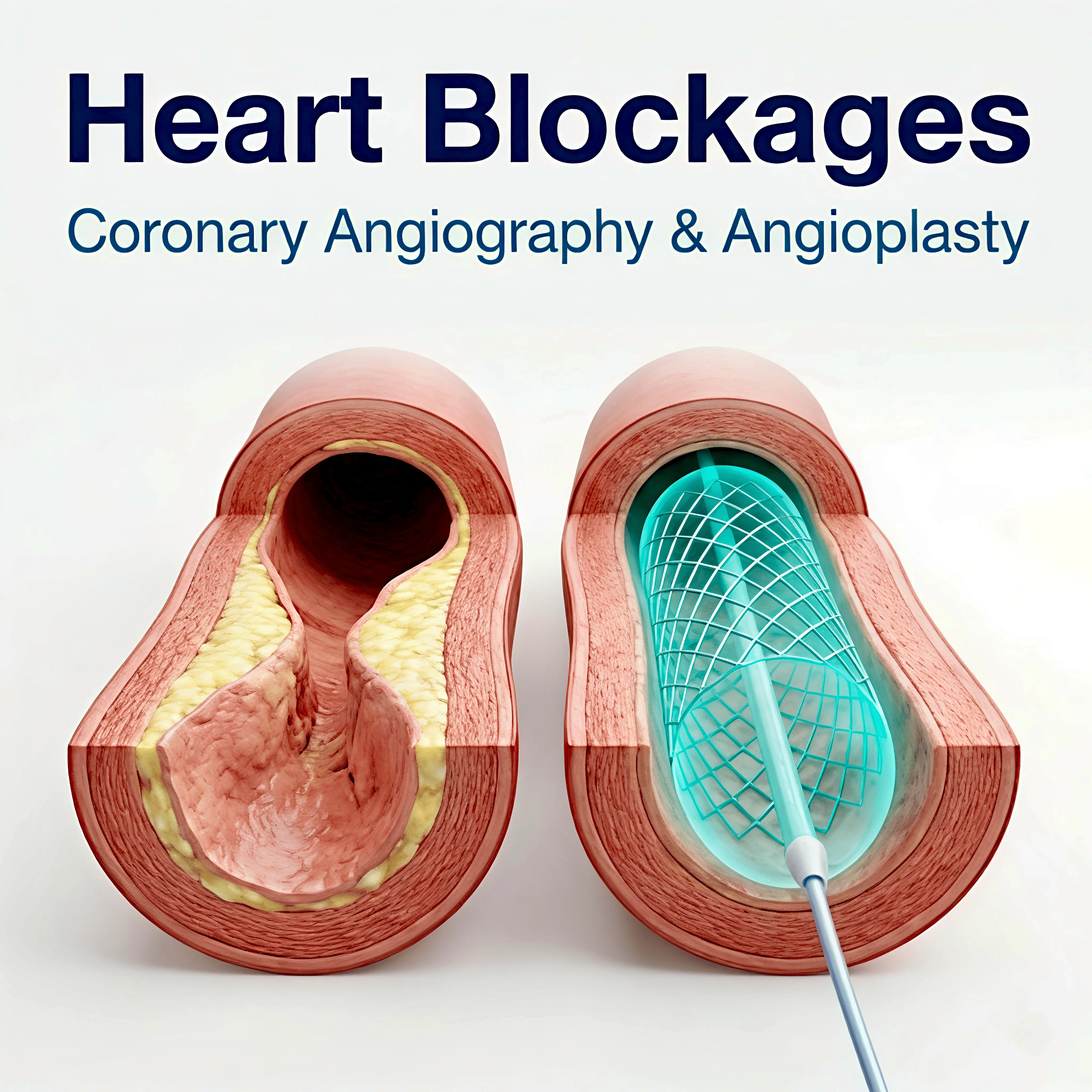
What Is a Heart Blockage?
The coronary arteries wrap around
the heart and supply it with blood. Over the years, fatty deposits - plaques -
build up on the inner walls of these arteries, narrowing them from the inside.
When this narrowing becomes significant, it restricts blood flow to the heart
muscle. This is what most people mean when they say 'heart blockage'.
Not all blockages are equal. A 50% narrowing behaves very differently from a 90% narrowing. And the same degree of narrowing can have very different implications depending on which artery is affected, where in the artery the blockage sits, and whether blood flow to the heart muscle is actually being compromised.
What Is
Coronary Angiography?
Coronary angiography is the
investigation used to visualise the coronary arteries in detail. A thin
catheter is guided through the wrist and up to the heart, where a contrast dye
is injected into the arteries under X-ray imaging. This produces a detailed
picture of where the arteries are narrowed, how severely, and how many arteries
are affected.
Angiography is highly accurate and
remains the gold standard for assessing coronary blockages before any decision
is made about treatment.
What Is Angioplasty and Stenting?
Angioplasty is the procedure used
to open a blocked or narrowed coronary artery. A thin catheter with a small
balloon on its tip is guided to the site of the blockage, usually through the
wrist. The balloon is inflated to push the plaque against the artery walls,
opening the vessel. In most cases, a stent, a small metal mesh tube, is then
placed to hold the artery open.
This is routinely done through the
wrist. There is no large incision, no general anaesthesia in most cases. Most
patients are mobile the same day and home the following morning. Within a few
days, many patients are back to their daily routine, walking, climbing stairs, and carrying on with their normal lives.
When Is a Stent Actually Needed?
This is the most important
question and one that most patients are not given the time to ask. A stent
placed where it is not clinically necessary adds risk without benefit. A stent
not placed where it is genuinely needed leaves a patient unprotected.
Our team uses IVUS (intravascular
ultrasound), which, where appropriate a technique that produces a detailed
cross-sectional image from inside the artery, giving a precise measurement of
how much the artery is genuinely narrowed. This removes subjectivity from the
decision and ensures we recommend intervention only when the evidence supports
it.
Second Opinion on a Blockage
If you have been told you have a blockage and are uncertain about the recommendation you have received, whether to have a stent, bypass surgery, or simply medications, our team is available to review your reports. Bring your angiography CD and any other investigations you have.
You
do not need a referral to come to Apollo CVHF. Bring your reports and we will
review them honestly. |